
The Imaging
Advantage
Standard angioplasty relies on 2D shadows. We put microscopic cameras inside the artery itself to achieve absolute, mathematical precision perfectly deployed for lifelong durability.
In Simple Terms
We don't guess your blockage — we measure it precisely before placing a stent. That single step changes everything.
Most angioplasties in India are done without advanced imaging. We don't take that risk.
"Precision is not an option; it is the standard. Guesswork has no place inside the human heart."

Inside The Artery
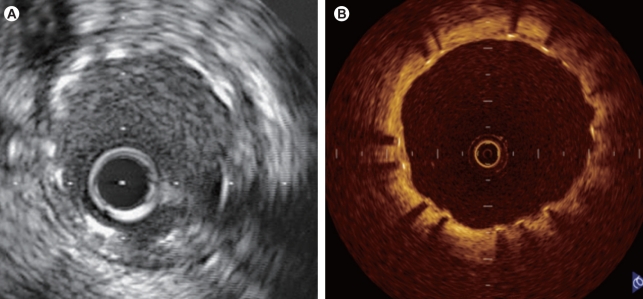
Intravascular Ultrasound (IVUS) and Optical Coherence Tomography (OCT) represent the pinnacle of interventional cardiology technology.
By inserting a microscopic camera or ultrasound emitter attached to a tiny catheter directly into the coronary artery, we generate a high-definition 360-degree view of your vessel wall from the inside out. This allows us to see exactly how much plaque exists, measure the exact diameter of the healthy vessel down to a fraction of a millimeter, and select the absolute perfect stent size.
IVUS
Ultrasound Soundwaves
Uses soundwaves to see deep into the vessel wall, measuring total plaque volume and identifying calcifications hiding under the surface.
OCT
Infrared Light
Uses near-infrared light for microscopic resolution, ensuring the stent struts are perfectly fused to the vessel wall without micro-tears.
2D Shadow vs 3D Reality
Below clip shows the inside of the vessel by OCT
OCT pull-back with real-time angiogram co-registration — OPTIS Integrated System
The "Zero Compromise" Philosophy
Why do some stents fail after five years, while others last a lifetime?
The vast majority of stent failures (restenosis or stent thrombosis) occur because the vessel was under-measured based on a 2D shadow, resulting in a stent that didn't expand fully against the arterial wall.
Why isn't everyone using this?
IVUS and OCT are time-consuming and require extensive specialized training. Routine cardiology often bypasses imaging to save time. Dr. Panda mandates imaging. We refuse to deploy a stent purely based on guesswork when a tool to verify mathematical precision exists. We verify the result from the inside.